

The Scapula
The Normal Scapula
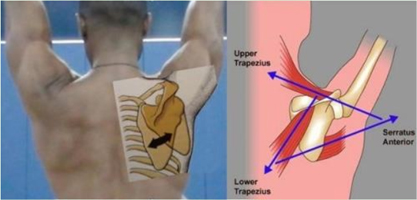
The scapula is a triangular bone and the outer (lateral) end of this bone is the socket of the shoulder joint. Normal movement of the scapula allows us to use the shoulder and arm in sports, work and daily living.
Upward and forward rotation allows us to raise our arms overhead. This is achieved by several muscles attaching to the scapula. The Serratus Anterior pulls the scapula forward and rotates the socket upward. The Trapezius rotates the scapula outward and the socket upward.
Scapulothoracic Dyskinesis
What is it?
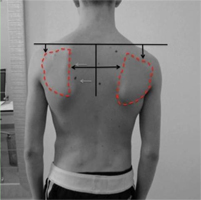
Scapulothoracic dyskenesis may be the result of fatigue of the scapular stabilizing muscles, and this may occur from overhead sports or work activities. Indeed, athletes with shoulder pain will often have abnormal scapular movement and this is an important part of their recovery with a physical therapy rehabilitation program. In its most severe form Scapulothoracic dyskenesis is the result of a nerve dysfunction either from trauma or idiopathic causes.
Loss of scapular control is often missed. The patient may develop pain in his(her) shoulder and there may or may not be loss of overall shoulder motion. In some cases the patient may have shoulder instability due to failure of the scapula to fully rotate.
Some patients present with pain that may seem like a rotator cuff problem. This is due to abnormal motion which allows the rotator cuff to hit against the acromion bone. This condition has been called impingement.
Scapulothoracic Winging
What is it?
If one or more of the scapular stabilizing muscles does not work properly the scapula wings and moves in the opposite direction of the shoulder joint. This results in limited motion.
Serratus Anterior Palsy
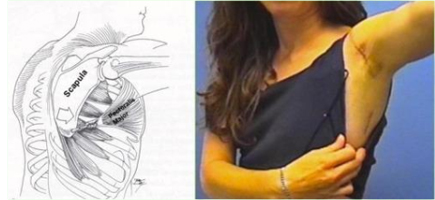
In the case of winging due to long thoracic nerve palsy (serratus anterior palsy), most cases recover but do so slowly and this may take up to one or two years for maximum recovery. Physical therapy is not generally helpful and may actually exacerbate winging by further stretching the long thoracic nerve
When winging due to Serratus Anterior Palsy persists and the patient is disabled and/or has pain, surgery is indicated. The most common solution is a pectoralis major transfer. The pectoralis major is transferred around the chest to the lower part of the scapula so it can substitute for the serratus anterior. Most surgeons use a tendon graft to lengthen the pectoralis tendon which may otherwise be too short. This graft typically is taken from the outside of the thigh (ilitibial band) or from the inside of the thigh(hamstring tendons).
Post op:
- The arm is in a sling for four weeks to allow the transfer to heal.
- Passive range of motion begins after the first 7-10 days.
- After four weeks the sling is removed and the patient is permitted to use the arm for simple daily living but no lifting.
- Physical therapy to restore flexibility continues. After 12 weeks biofeedback training may be added to the therapy program to help train the tendon to contract as the arm is raised.
Trapezius Palsy
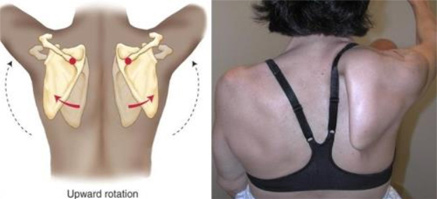
A less common form of winging that may also result in weakness and pain. The trapezius is a very large triangular muscle which supports the scapula suspending it from the spine and the neck. It works to rotate the scapula outward to the side and upward so that the glenoid socket points up allowing for the arm to be raised overhead out to the side. It also helps an individual shrug their shoulder.

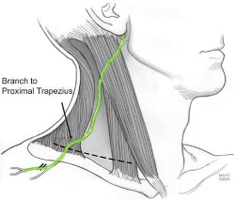
When it is not functioning properly the shoulder appears to droop downward and the scapula cannot rotate outward so the glenoid socket points downward and the patient is unable to raise the arm. The nerve which makes the trapezius work is the spinal accessory nerve. It is typically injured as the result of a direct trauma as in an auto accident or from a penetrating injury such as a surgery.

If the patient has a significant disability and pain then a tendon transfer may be a solution. The tendon transfer is called the Eden-Lange procedure and it involves transfer of several muscles. The levator scapula, the rhomboid major, and the rhomboid minor are transferred so as to have a similar orientation of the trapezius so they can substitute for its loss of function.
Post op:
- The shoulder is protected in a sling for 4 weeks after which active and passive motion begin.
- Lifting is avoided for 4 months after surgery.
- Results of the Eden-Lange Procedure for trapezius palsy are generally good with most patients noting improved motion and pain relief.
Combined loss of function
The third type of winging occurs when there is a combined loss of function of the serratus anterior and the trapezius muscles. This usually associated in a conditional called Fascioscapulohumeral muscular dystrophy (FSH). Patients may present with weakness so severe they are unable to raise the arm either forward or to the side.
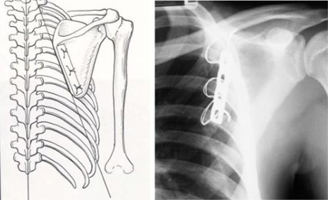
In such cases, or when a tendon transfer has failed, there may be no tendon transfer solution. For these patients a fusion of the scapula to the ribs (scapulothoracic fusion) may give stability to the scapula which allows the patient to raise his(her) arm overhead
Post op:
- The shoulder is immobilized in a sling for up to 12 weeks.
- During this time elbow, wrist, and hand motion is permitted.
- Once a solid fusion is evident (usually on a CT scan) the patient is permitted to move the shoulder and begin therapy.
