

Elbow Instability
The elbow is both a hinge joint and a ball and socket joint between the humerus in the upper arm and the radius and ulna in the forearm. If the humerus slips out of the depressions in the radius and ulna, this may lead to dislocation or instability.
Anatomy
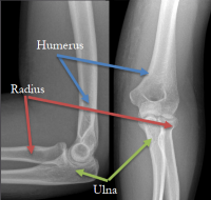
The elbow joint: The elbow joint is comprised of the three bones of the arm - the humerus in the upper arm and the ulna and radius of the forearm. The rounded ends in the front side of the humerus, the trochlea and capitulum, sit in the shallow depressions in the ulna (coronoid notch) and the radial head, respectively. This allows for the hinging motion of the elbow as well as some rotation as the hand is rotated palm up and palm down. The extension of the arm is limited as a long process in the back of the ulna, the olecranon process, catches in a shallow depression in the back of the humerus, the olecranon fossa, locking the elbow joint in place as the arm straightens.
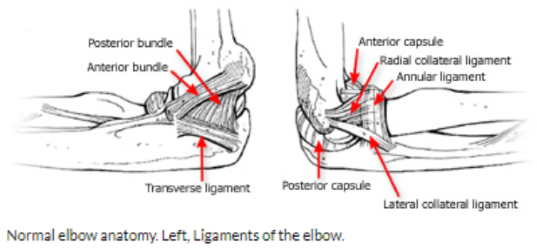
Stabilizing the joint: The elbow joint is encased in the front and back by the joint capsule, strong connective tissue, comprised of ligaments, which stabilizes the joint. Muscles which cross and attach near the joint add stability to the elbow. Two important strong ligaments, the collateral ligaments, significantly work to hold the joint together as they run across the elbow. The lateral collateral ligament (on the outside border of the elbow if the palm is up) and the ulnar collateral ligament (on the inside border of the elbow if the palm is up) prevent dislocation.
Causes
Elbow instability is a looseness in the joint that causes catching, locking, popping, and sliding sensations. This may occur due to dislocation or subluxation- when the humerus slips entirely or partially out of the depressions where it sits in the ulna and radius. This may be result of a traumatic event or injury.
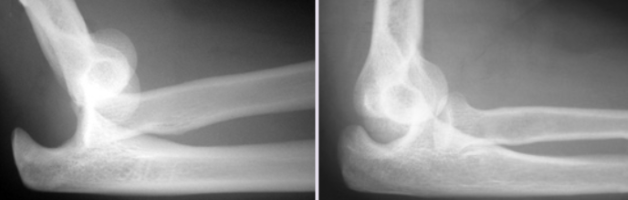
X-Rays showing a complete elbow dislocation (left) and partial elbow dislocation, or subluxation (right)
Recurrent instability may be a consequence of injury to the ulnar or lateral collateral ligaments with or without a fracture to one of the bones comprising the elbow. Injury to the ligaments may be caused by trauma such as a fall, previous surgery, repetitive stress (such as that for overhead athletes like baseball pitchers), or an existing elbow deformity. Three types of recurrent instability:
- Posterolateral rotatory instability: Most common, caused by trauma which damages the lateral collateral ligament complex. Characterized by a sensation of sliding in orout.
- Valgus instability: Caused by injury to the ulnar collateral ligament complex.
- Varus posteromedial rotatory instability: Caused by injury to the lateral collateral ligament complex in addition to fracture of the coronoid of the ulna. Typically caused by a trauma. Characterized by sensation of sliding in or out.
Symptoms
Symptoms of instability include pain as well as sensations of catching, locking, popping, clicking, or sliding of the elbow. There may also be a sense that the elbow may pop out of place, particularly when pushing yourself out of a chair.
Diagnosis
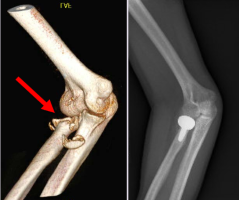
Elbow with lateral instability caused by a traumatic fracture and dislocation after realignment. A fracture of the radial head (red arrow) was repaired with a radial head replacement (seen in X-ray on the right).
Through physical examination, doctors can assess for tenderness, deformity, and for locking or catching sensations while moving the arm. Diagnosis of injuries to the bone and soft tissue which may be underlying the instability can be made through X-rays and Magnetic Resonance Imaging (MRI), respectively.
Non-surgical treatments
Non-surgical treatments of elbow instability include physical therapy for strengthening the muscles around the joint, activity modification to avoid pain or sensations of instability, a brace to stabilize the elbow in place, and pain management. Elbow dislocations can be treated non-operatively by reducing the elbow back into alignment, which may be done in a doctor’s office or emergency department, followed by a brace, pain management, and, eventually, physical therapy.
Surgical treatments
Elbow instability may be treated by reconstruction of the injured ligaments with a tissue graft, either from one of the patient’s own ligaments or an allograft harvested from a cadaver. If a fracture to the bone has occurred, the fragments can be realigned and fixed into place with screws or a plate.
Complex elbow dislocations may require surgery to realign the elbow. The elbow may be fixed with an external hinge and any damage to nerves, ligaments, or blood vessels around the elbow are repaired. Surgery may also be necessary to remove scar tissue and extra bone growth if the elbow stiff remains after realignment.
Sources: American Academy of Orthopaedic Surgeons, Ortho Info, “Reccurent and Chronic Elbow Instability” and “Elbow Dislocation”
