

Distal Triceps Repair
Prevalence of Biceps rupture

- Fall on the hand with elbow in extension
- Sports1
- Excessive load
- Weightlifters and athletes2
- Patients with diseases involving collagen structure and tendon quality3
- Ex. rheumatoid arthritis, Marfan's syndrome
- Patients undergoing elbow arthroplasty3
- http://pathologies.lexmedicus.com.au/pathologies/radial-head-fracture
- https://www.bodybuilding.com/content/6-best-triceps-workouts-for-men.html
- Sollender JL, Rayan GM, Barden GA (1998) Triceps tendon rupture in weight lifters. J Shoulder Elbow Surg 7(2): 151-153.
- Mair SD, Isbell WM, Gill TJ, Schlegel TF, Hawkins RJ (2005) Triceps Tendon Ruptures in Professional Football Players. Am J Sports Med 32(2): 431-434.
- Demirhan M, Ersen A. Distal triceps ruptures. EFORT Open Rev. 2017;1(6):255–259. Published 2017 Mar 13. doi:10.1302/2058-5241.1.000038
Anatomy of Triceps

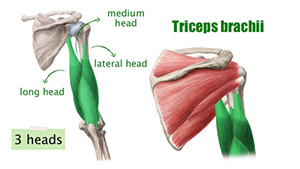 Consisting of 3 muscular heads that gather into a single insertion on the olecranon
Consisting of 3 muscular heads that gather into a single insertion on the olecranon
- long head
- lateral head
- medial head
- Presence of distinct footprint areas in the olecranon for
- posterior elbow capsule
- medial head of the triceps
- common tendon of the long and lateral head of the triceps
Triceps Insertion




Area: 466 mm2
Width: 1.6 – 4.2 cm
Starts 12 mm from olecranon tip
Primary Acute Repair Technique Complete and Partial
- Complete ruptures should always be treated surgically
- Partial ruptures can be treated conservatively or surgically
- Surgical repair recommended when patient experiences loss of strength or is symptomatic
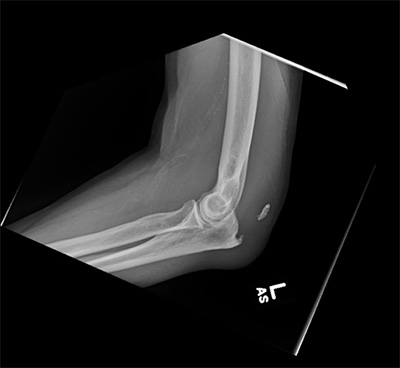
Case Example–
- Patient history
- 73 yr old gentleman elbow injury while swinging golf club
- Constant dull elbow pain and weakness
- Inability to workout and play golf
- Clinical examination
- Palpable defect
- Marked weakness with elbow extension
Imaging
Methods of Repair - Transosseous bone tunnel Repair


- Bunnell technique
- Krakow technique
- Suture and wire
 Krakow locking-type sutures placed through drill holes
Krakow locking-type sutures placed through drill holes Bunnell Technique
Bunnell Technique
Methods of Repair - Suture Anchor Repair
- Triceps Pulley-Pullover Technique
- Double Row Repair
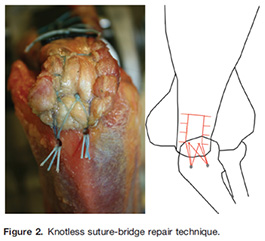
- Knotless
- Knotted
 Suture Anchor placement
Suture Anchor placement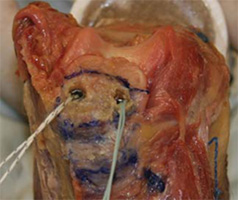 Suture Anchors
Suture Anchors Double Row technique
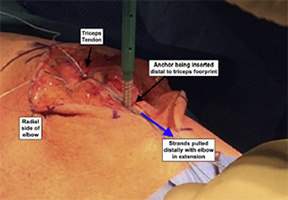
Double Row technique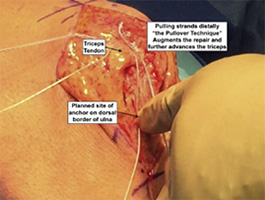 Pull-over technique
Pull-over technique

- Combination technique using drill holes & single suture anchor

Outcomes from Distal Triceps Tendon Repairs
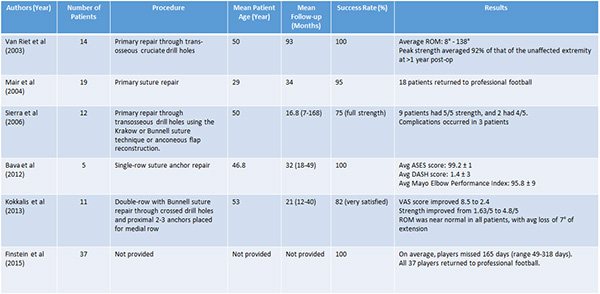
Outcomes from Distal Triceps Tendon Repairs
- Primary repair: Good outcomes (strength and function) in majority of patients.
- Low complication and re-rupture rates.
- No differences between technique/method of repair!
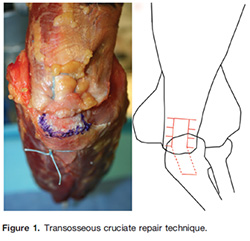
What about Biomechanical Evidence?

- No significant difference in post-procedure biomechanical strength between transosseous cruciate repair and suture anchor repair.
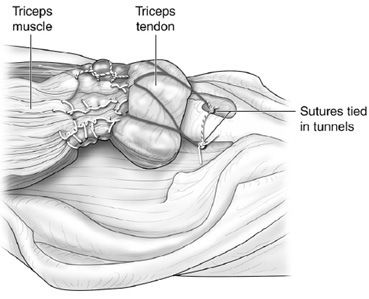 Final Transosseous cruciate repair construct
Final Transosseous cruciate repair construct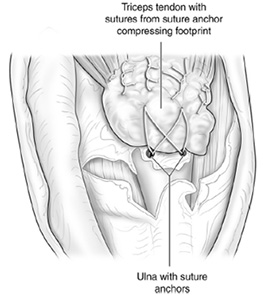 Final suture anchor construct
Final suture anchor construct

- Distal triceps knotless anatomic footprint repair resulted in greater biomechanical strength and resistance to displacement at the tendon-bone interface compared to traditional transosseous cruciate repair.
 Knotless Anatomic footprint final fixation
Knotless Anatomic footprint final fixation

- Transosseous cruciate techniqueWeakness Construct
- knotless suture-bridge technique
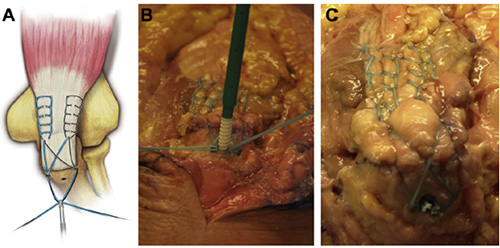
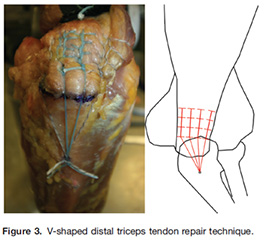
- V-Shaped Techniquehighest load to failure
Bottom Line
- Suture anchor augmented repair probably biomechanically superior to traditional transosseous repair.
- Any technique can work if executed well!
My Preferred Setup & Equipment
- Supine (Arm holder or bump)
- Lateral with arm holder
- Suture Anchors
- 3.0 double loaded suture anchors for proximal row (two anchors)
- 4.5-5.0 mm knotless suture anchors for lateral row (two anchors)
- No C-arm necessary for primary repair
- Rongueur to prepare olecranon, no burr needed
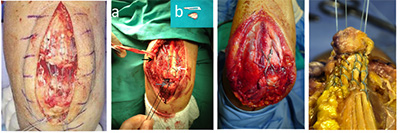
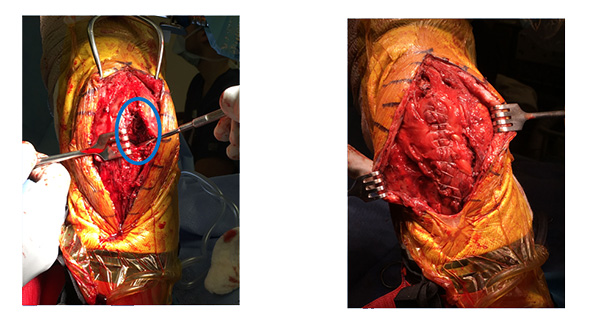
Double Row Surgical Technique
Case Study – Triceps Repair
2 Year Outcome
Pros- Cons Suture Only vs Suture Anchor
Suture Only
- Decreased Cost
- Less strong repair
- Slower Rehab?
- Low fracture risk
Suture Anchor
- Increased Cost
- Stronger Repair
- Faster Rehab?
- Increased fracture risk?
Pearls of Treatment
- Look for fleck sign - use it to your advantage and don’t excise it
- Don’t place your incision directly over the olecranon process!
- Beware of the Ulnar nerve!
- Use a hinged elbow brace to protect the repair
How To Rehab?
- Splint 60-90 degrees posterior slab plaster splint for 10 days
- Transition to hinged elbow brace
- Increase flexion by 30 per week
- Passive/gravity extension and active flexion
- At 8-12 weeks depending on patient and repair factors may begin light strengthening
- Typically 6-12 months before return to play depending on sport/demands
Chronic/Failed Triceps Repairs
Case Example
- 50 yr. old male carpenter presented with right elbow pain and swelling
- A history of 3 prior repair surgeries (approx 12 months since last surgery)
- Pain, weakness and symptomatic bursitis
- Performed olecranon bursectomy and revision repair with suture anchors
- However, patient developed increased pain in the weeks afterwards and reported several instances of elbow swelling
Imaging

Revision/Chronic Triceps Reconstruction Options
- Two basic ideas:
- Salvage with various rotational flaps
- Reconstruction with allograft/autograft tissue
- Achilles tendon reconstruction
- Semitendinosus reconstruction
Reinforcement with a reflected slip of fascia from the posterior forearm
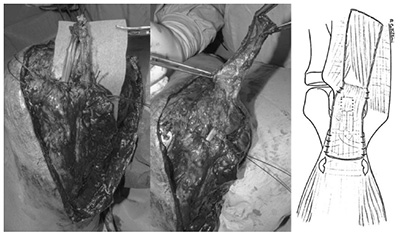 Tendon graft passed through bone tunnels and reinforced using flap of fascia detached from forearm
Tendon graft passed through bone tunnels and reinforced using flap of fascia detached from forearm
Use of Flaps
- Anconeus Muscle Rotation Flap
- Triceps Tendon Flap
- Olecranon periosteal flap
 Anconeus Rotation Flap
Anconeus Rotation Flap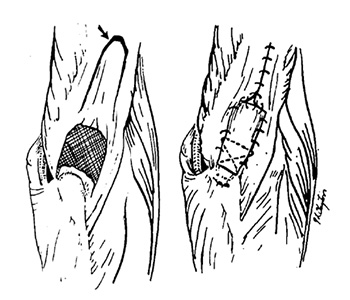 Triceps Tendon Flap (Patient with Olecranon Bursitis)
Triceps Tendon Flap (Patient with Olecranon Bursitis)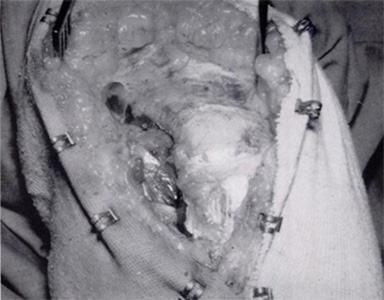 Olecranon periosteal Flap
Olecranon periosteal Flap

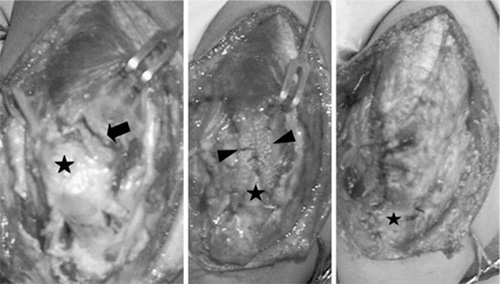 Use of musculotendinous/periosteum sleeve
Use of musculotendinous/periosteum sleeve
Methods of Repair - Achilles tendon allograft

 Proximal suture of the allograft
Proximal suture of the allograft Completed proximal suture of the allograft
Completed proximal suture of the allograft

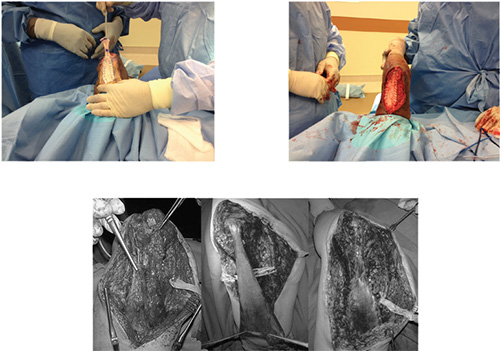
 Triceps tendon reconstruction with semitendinosus graft
Triceps tendon reconstruction with semitendinosus graft

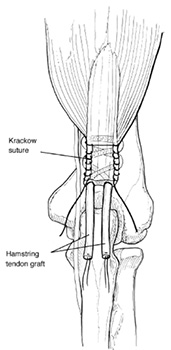 Semitendinosus grafts woven through triceps
Semitendinosus grafts woven through triceps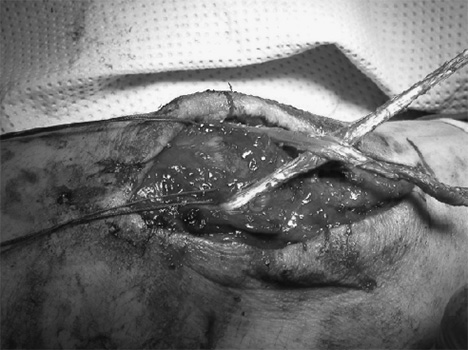 Hamstrings graft
Hamstrings graft

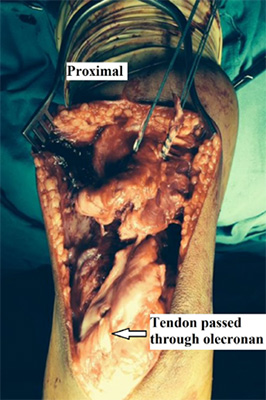
 Transosseous tunnels and anchor positioning
Transosseous tunnels and anchor positioning Final suture construct
Final suture construct
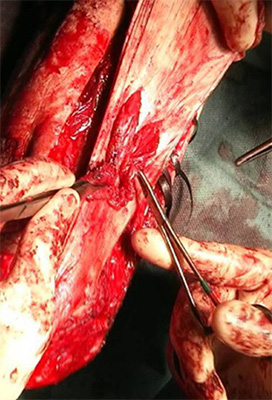
 Autograft tendon woven through triceps tendon using Bunnell technique
Autograft tendon woven through triceps tendon using Bunnell technique
Autograft Semitenidonsus & Gracillis Recon – Docking Technique
Autograft Semitenidonsus & Gracillis Recon – Docking Technique

3 Year Outcome
Reconstruction Pearls
- For athletes/high demand be prepared to perform reconstruction
- Anticipate tissue loss
- Use autograft
- Consider anatomic repair
- Match the reconstruction with the tissue loss
Case Study
- 37 y.o. right hand dominant male
- Avid weightlifter
- History of failed prior triceps repair
- Presents with left elbow pain from lifting weights
- Pain is 7/10 at worst, 4/10 on average
- Has been treated with anti-inflammatories and rest
- Exam
- ROM 0° to 130°
- 90°/90° pronation/supination
- Tender to palpation over distal triceps
- 4/5 strength with elbow extension, 5/5 with flexion
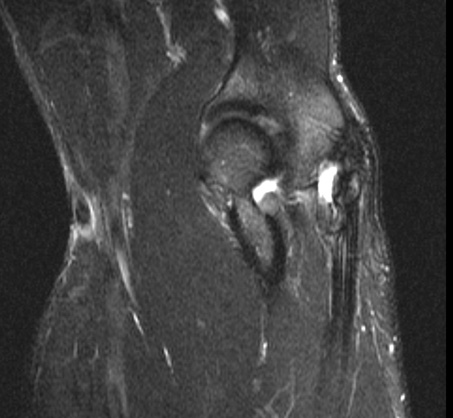
Case Study
- Obtained x-rays and MRI
- X-rays show osteophytes or HO involving distal triceps
- MRI scan shows partial tear of the triceps with 1.9cm of retraction
Case Study
- Elected to proceed with a left elbow triceps repair
- At one year follow-up, patient has made excellent progress
- Lifting weights without restriction
- No pain
- ROM from 0° to 130°
- 5/5 triceps strength
