

Distal Biceps Repair
Prevalence of Biceps rupture
- Excessive eccentric tension as arm is forced from flexed to extended position1
- weightlifting, wrestling and labor intensive job2
- Greater risk in patients who smoke (7.5 times)1,3
- Higher BMI3
- Presence of rotator cuff disease4
- Safran MR, Graham SM (2002). Distal biceps tendon ruptures: incidence, demographics, and the effect of smoking. Clin Orthop Relat Res. 404):275-83.
- Thomas JR, Lawton JN (2017). Biceps and Triceps Ruptures in Athletes. Hand Clin. 33(1):35-46
- Kelly, M. P., Perkinson, S. G., Ablove, R. H., & Tueting, J. L. (2015). Distal Biceps Tendon Ruptures: An Epidemiological Analysis Using a Large Population Database. The American Journal of Sports Medicine, 43(8), 2012–2017. https://doi.org/10.1177/0363546515587738
- Vestermark GL, Van Doren BA, Connor PM, Fleischli JE, Piasecki DP, Hamid N (2018). The prevalence of rotator cuff pathology in the setting of acute proximal biceps tendon rupture. J Shoulder Elbow Surg. 27(7):1258-1262.
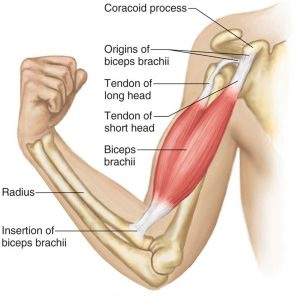
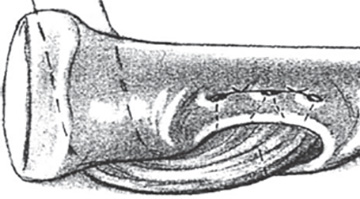
Anatomy of Biceps
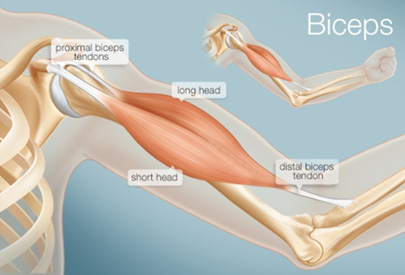 Consisting of 2 muscular heads that gather into a single insertion on the radial tuberosity and the fascia of the forearm
Consisting of 2 muscular heads that gather into a single insertion on the radial tuberosity and the fascia of the forearm
- long head (caput longum)
- short head (caput breve)
 Presence of distinct footprint areas
Presence of distinct footprint areas
- Biceps Tendon Footprint
Biceps Insertion

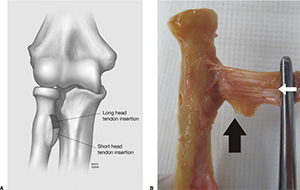 Area: 108 mm2
Area: 108 mm2
Width: 6 – 10 mm (Avg: 7 mm)
Length: 17 – 25 mm (Avg: 21 mm)
Starts 23 mm from the articular margin of the radial head
Primary Acute Repair Technique Complete and Partial
- Complete ruptures should always be treated surgically unless medically not indicated.
- Partial ruptures can be treated conservatively or surgically
- Surgical repair recommended when patient experiences loss of strength or is symptomatic
Is nonoperative management of partial distal biceps tears really successful?


- 55.7% of patients who tried non-operative treatment ended up undergoing surgery.
- High-need patients (defined by occupation) were more likely to report that they recovered ideally if they underwent surgery (OR: 11.57, p = 0.0138).
- MRI-diagnosed tear of > 50% was predictor of needing surgery.
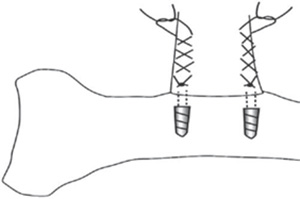
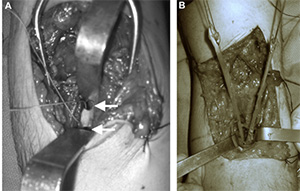
Methods of Repair – Two Incision Transosseous bone tunnel Repair


 Sutures passed and tied across bone bridge, via posterior incisions
Sutures passed and tied across bone bridge, via posterior incisions
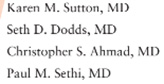
Methods of Repair – Single Incision-Suture Anchor Repair

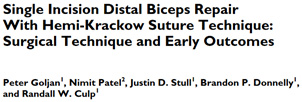


 Double Anchor placement
Double Anchor placement Bilateral Krakow Stitching
Bilateral Krakow Stitching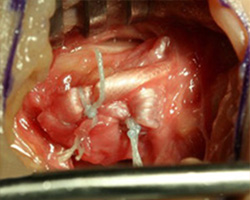 Tendon repaired to Tuberosity
Tendon repaired to Tuberosity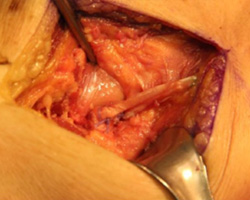 Repair using Hemi-Krackow Suture Technique
Repair using Hemi-Krackow Suture Technique
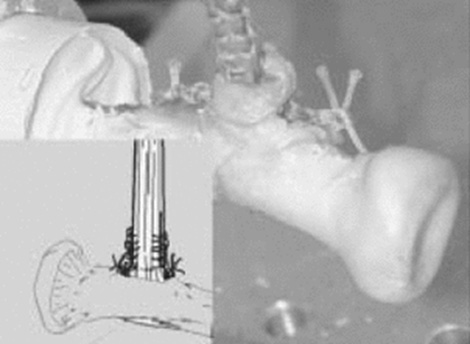
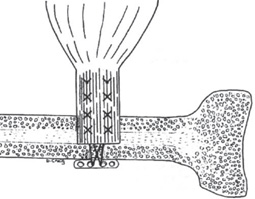
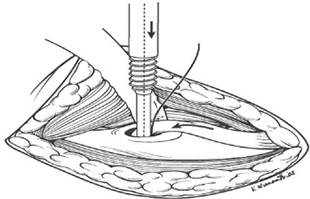
Methods of Repair - Interference Screw Fixation

- Bio-absorbable Tenodesis Screw
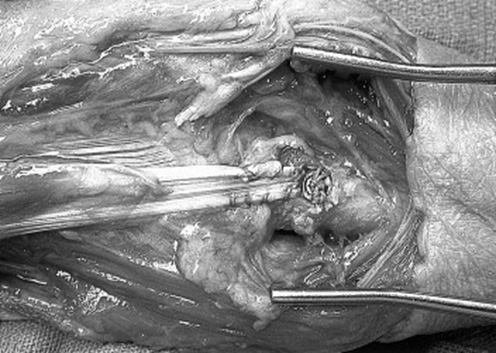 Distal biceps repair via Bio-Tenodesis screw
Distal biceps repair via Bio-Tenodesis screw




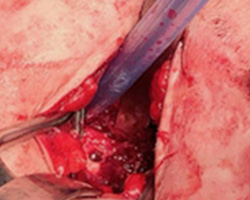 Unicortical drill hole
Unicortical drill hole Distal End of Biceps is whipstitched
Distal End of Biceps is whipstitched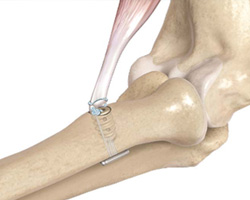 Cortical Button with Inference Screw
Cortical Button with Inference Screw Suture threaded through button
Suture threaded through button Sutures passed through Endobutton
Sutures passed through Endobutton
and then passed through biceps tendon Suture limbs tied over interference Screw
Suture limbs tied over interference Screw
Single vs. Double Incision Techniques


- Overall frequency of reported complications is higher for single-incision repair.
- Frequencies of re-rupture and nerve complications are both higher for single-incision repairs.
- Frequency of heterotopic ossification is higher for double-incision repair.
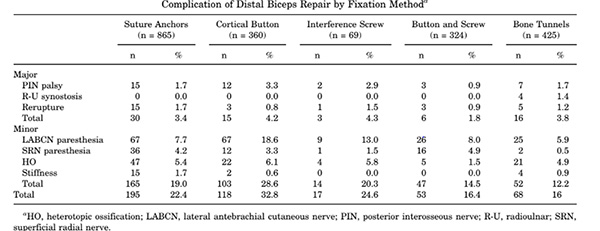
Outcomes from Distal Biceps Tendon Repairs

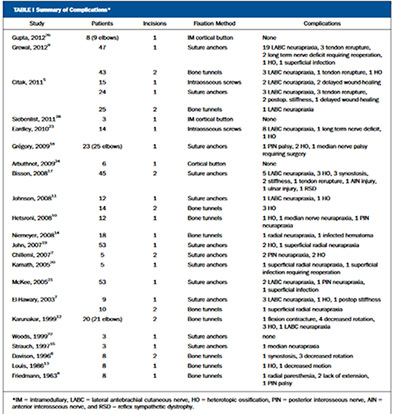
- 22 studies, 498 elbows
- Complication rate 25% (122 of 498 elbows)
- No difference:1 & 2 incision techniques
- 26% suture anchors
- 20% bone tunnels
- 45% intraosseous screws
- 0% cortical button fixation
- Most common complication
- LABC neurapraxia :9.6% across all studies
- 11.6% for one incision
- 5.8% for two incisions
- LABC neurapraxia :9.6% across all studies

Outcomes from Distal Biceps Tendon Repairs
- Primary repair: Good outcomes (strength and function) in majority of patients.
- Low rates of major complications
- Low re-rupture rates.
- No differences between technique/method of repair!
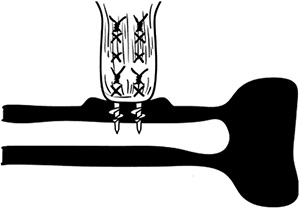
What about Biomechanical Evidence?
- Mean pullout strength of the repair with a Bio-Tenodesis screw was significantly higher, compared to suture anchors.
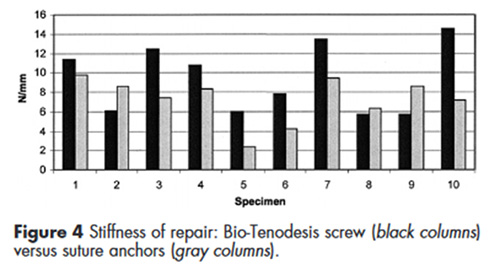


Suture anchor fixation resulted in greater yield strength compared to bone tunnel fixation.
 Suture Anchor Fixation
Suture Anchor Fixation
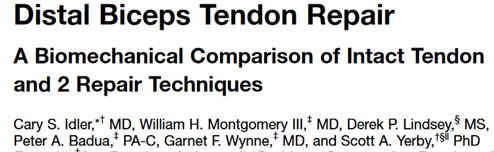
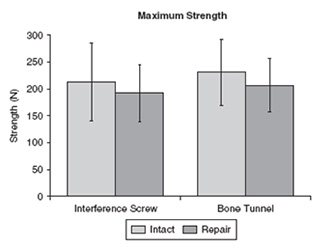
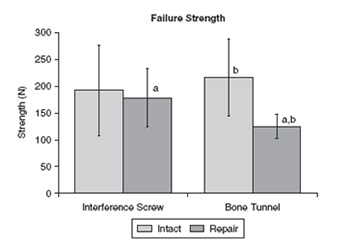
- Mean failure strength and stiffness: tunnel < interference screw < intact Specimens
- No significant differences between intact a& interference screw
- Interference screw fixation repair is nearly as strong and stiff as the intact tendon and stronger than the bone tunnel repair technique.

- No differences in final displacement between suture anchor group and EndoButton group
- Comparable fixation strength
 Schema of suture anchor repair
Schema of suture anchor repair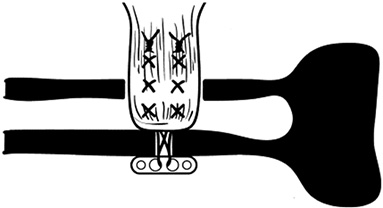 Schema of EndoButton sutured to tendon
Schema of EndoButton sutured to tendon
- Greatest Load to FailureEndoButton Repair
- Suture Anchor Repair
- Bone-Tunnel Repair
- Lowest Load to FailureInterference Screw Repair
Bottom Line
- Mixed results in biomechanical studies
- My interpretation: cortical button repair with interference screw superior to any other repair technique.
- Any technique can work if executed well!
Revision/Chronic Biceps Reconstruction Options
Reconstruction with allograft/autograft tissue
- Achilles tendon reconstruction
- Semitendinosus reconstruction
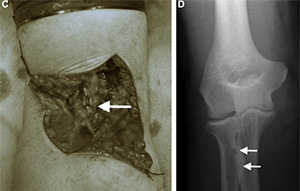
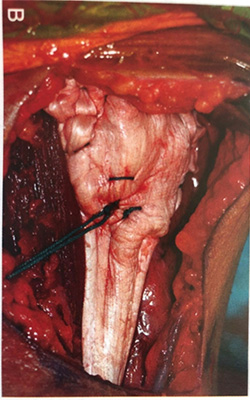
Methods of Repair - Achilles tendon allograft

Case Study - Chronic/Failed Biceps Repairs
Case History
- Patient history
- 47 yr. old male w/a history of left distal biceps tendon rupture.
- Originally taken to OR a few months prior but surgeon at the time was unable to preform repair due to short tendon
- Pt. rates elbow function as 30% and pain as 3/10
- Clinical examination
- Elbow range of motion is 5-135°
- 80–80 pronation supination
- Weakness with resisted forearm supination
- stump of the tendon is not easily palpable.
- Tender palpation over the antecubital fossa.
- Absent distal biceps tendon
Pre-operative motion
Imaging


MRI
My Preferred Setup & Equipment
- Supine with arm board
- Small C-Arm
- Suture button plus PEEK (non-absorbable) interference screw
- Single transverse incision directly over radius
- Optional – second transverse incision biceps tendon origin
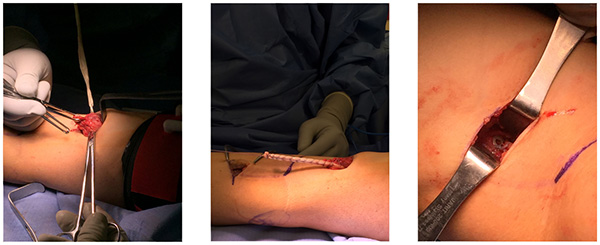
Procedure

2.5 Year Outcome

2.5 Year Patient Outcomes
- Pt. reported noticeable improvement in ROM and pain.
- Still some weakness with activity but generally can do most all activities
- SANE 80%, Pain 2-3/10
- Pt. was satisfied with outcomes and reports general improvement in function.
- Returned to work as a laborer
Reconstruction Pearls
- Anticipate tissue loss
- Autograft vs allograft?
- Match the reconstruction with the tissue loss
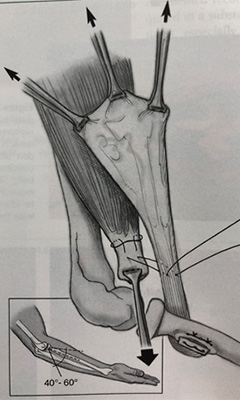
- With allograft fix with elbow in 45 degree of flexion- will stretch out
- Use fluoroscopy to verify location of incision, drill hole and deployment of button
Pearls of Treatment
- Use small c-arm to localize location of incision, verify location of drill hole and verify deployment of button.
- Beware of the LABC and PIN nerves! Identify and dissect free the LABC & avoid using Homan retractors on radial aspect of radius.
- Use a hinged elbow brace to protect the repair if tension requires more than 30-45 degrees of flexion
